Neurodyn Aussie Sport transcutaneous neuromuscular stimulator is a four-channel stimulator with independent controls for electric current therapy used in AUSSIE CURRENT (Burst Modulated Medium Frequency).
Aussie current (Australian Current) is a medium frequency alternating electric current released in short bursts (1 kHz/ duration of Burst of 2 ms or 4 kHz/ duration of burst of 4 ms) used to produce respectively maximum muscle torque or analgesia, without significant discomfort for the patient.
The equipment is for use only under the prescription and supervision of a licensed professional.
Output mode: Electrodes
Intensity (CC): 0-120 mA* ±20%
Frequency of carrier (Carrier): 1 or 4 kHz ±10%
Duration of Burst (Burst ms): 2 or 4 ms ±10%
Current modes (Mode):
Continuous (Cont) 1, 2, 3 or 4 channels
Synchronous (Sync) 1, 2, 3 or 4 channels
Reciprocal (Rec) 1 and 3; 2 and 4 channels
Sequential (Seq) 1, 2, 3 or 4 channels
Frequency of Burst (Burst Hz): 1-120 Hz ±10%
Ramp:
Duration of up ramp (Rise): 1-20 s ±10%
Duration of muscle contraction (On):1-60 s ±10%
Duration of down ramp (Decay): 1-20 s ±10%
Duration of muscle relaxation (Off): 1-60 s ±10%
Treatment duration (Timer): 1-60 min ±10%
Intensity Control (UP or DOWN): Individual channels of intensity 1, 2, 3 and 4
* Load Impedance range for these parameters: 800-1200 Ohms.

In recent years the use of electric currents to treat various tissue dysfunctions and their symptoms, has been quite intense. Inflammatory conditions can be controlled and reduced, pain can be modulated until the cause of pain is eliminated, tissue repair can be achieved quickly and muscle function can be restored. Reports about the use of excitomotor electric currents in professional athletes have been made and the performance increase as well as neurophysiological, morphological and biochemical alterations reported by researchers.
Commercially RUSSIAN electric current, Interferential and FES (Functional Electrical Stimulation) are classic, however, until now there has been no intense concern to develop and produce new treatment options using electrical currents that provides comfortable sensory stimulation without compromising electrophysiological efficiency as well as a powerful motor stimulation without reaching the painful threshold and thus, the evolution of neuromuscular electrical training is limited due to the presence of pain caused by the stimulation itself.
Researches have recently suggested that alternating electric currents modulated in long-duration Burst produced by traditional electric currents such as Russian and Interferential are not the best way to minimize discomfort during sensory stimulation and to produce high levels of muscle torque during motor stimulations. The 4000Hz or 4kHz frequency of modulated alternating currents in short bursts offers less discomfort during sensory stimulation. Interferential therapy uses this carrier current value, however, its modulation in Bursts is very long. The Australian electric current has the capacity to perform sensory stimulation with minimal discomfort as it is also a medium frequency electric current (4000Hz or 4kHz) and also due to the use of short-duration Burst modulation, making it even more comfortable. when compared to interferential therapy and Russian electric current.
Studies also suggest that for intense and efficient motor stimulation with minimal discomfort the frequency of 1000Hz or 1kHz must be combined with modulation in Bursts lasting 2 ms. This is the Australian electric current for functional recovery of skeletal muscles.
Resistance to muscle fatigue is an extremely important factor within rehabilitation procedures involving the recovery of skeletal muscles, particularly when using an excitomotor electric current (FES, Russian, Interferential). For FES, it is important to minimize muscle fatigue. The accumulation of electrical stimulus can become a problem when using medium frequency alternating electric currents, especially if the modulation in Burst is long. In this case, the nerve fibers may suffer accumulation of electrical current in the fiber reaching the threshold and thereafter suffer repolarization and depolarization again, during the same burst. Thus, this accumulation can result in neural fiber depolarization at the beginning of Burst and then the nerve fiber may then not recover enough and shoot again. If the bursts present long lasting there will be great potential for the nerve fiber to be shot several times within the same burst.
Thus, if the Bursts are too long, as in Interferential Therapy and Russian current, there is a high risk of multiple shoots or depolarization of Alpha motoneurons within the same Burst. Then it is suggested, modulation frequencies in 40HZ as superior values may lead to a premature muscle fatigue.
The use of the Australian Current for motor stimulation allows higher levels of muscle torque and even lower occurrence of muscle fatigue. Burst duration is kept short to prevent multiple shots of Alpha motoneurons
Australian electric current is structured by short Bursts separated by long time intervals and therefore the skin irritation risks are short because the electric current density is reduced. Anyway, bigger electrodes are ideal as a result of less discomfort provided through the reduction of the electric current density and less nociceptive stimulation.
A more recent study by McCarthy (2007) compared the Australian electric current to a pulsed electric current and found that the first one was more comfortable and also more efficient. The short duration of bursts from electric current results in high efficiency during analgesia procedures without compromising the most pleasurable sensation during therapy. A similar study by Ward and Oliver (2007) compared low frequency pulsed electric current to the Australian electric current for analgesia and once again found greater efficiency with less discomfort with the Australian electric current compared to T.E.N.S.
Thus, evidence indicates that when using an alternating electric current with frequency in the kHz range modulated in short duration Bursts, the analgesia effect is better when compared to a T.E.N.S. The stimulation is more comfortable and the tolerance level of the patient increases considerably, which makes the treatment more efficient
The Australian electric current is a physical therapeutic resource that is born to add clinical value to the care provided to patients who need physical rehabilitation in several areas of physiotherapy. It is important to emphasize that several scientific publications give unquestionable support to the efficiency of the use of the Australian electric current, a situation that has not been verified during the conception of other electrotherapeutic resources over the years. All the physical values attributed to the Australian electric current both for muscle reinforcement as for sensory stimulation have a vast scientific basis and so, for this therapeutic modality the practice based on evidences is an undeniable reality.
Relaxation of muscle spasms.
Prevention or retardation of disuse atrophy in post-injury type conditions.
Increase local blood circulation.
Muscle re-education.
Maintaining or increasing range of motion.
Symptomatic relief of chronic intractable pain.
Post-traumatic acute pain.
Post-surgical acute pain.
Adverse reactions
After the procedure, it is common that the patient presents Hyperemia (in some cases, a slight emaciation) and hypersensitivity.
Patients may present skin irritation or hypersensitivity caused by electrical stimulation or means of electrical conduction. The irritation can usually be reduced with the use of an alternative mean of conducting or with the placement of an alternative electrode.
Patients may present skin burns under the stimulation with electrodes if the application is not correctly carried out or if the electrodes are worn out.

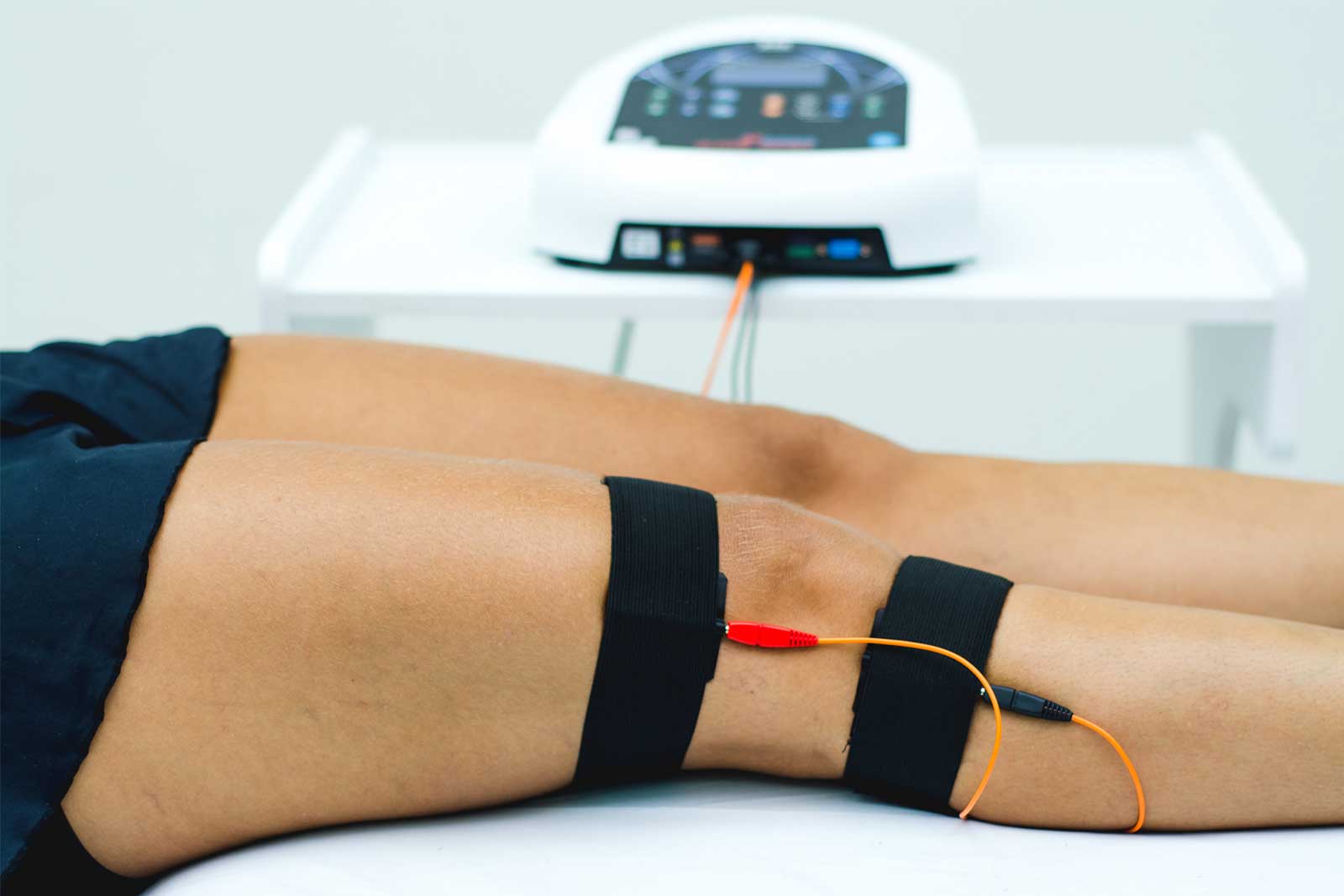
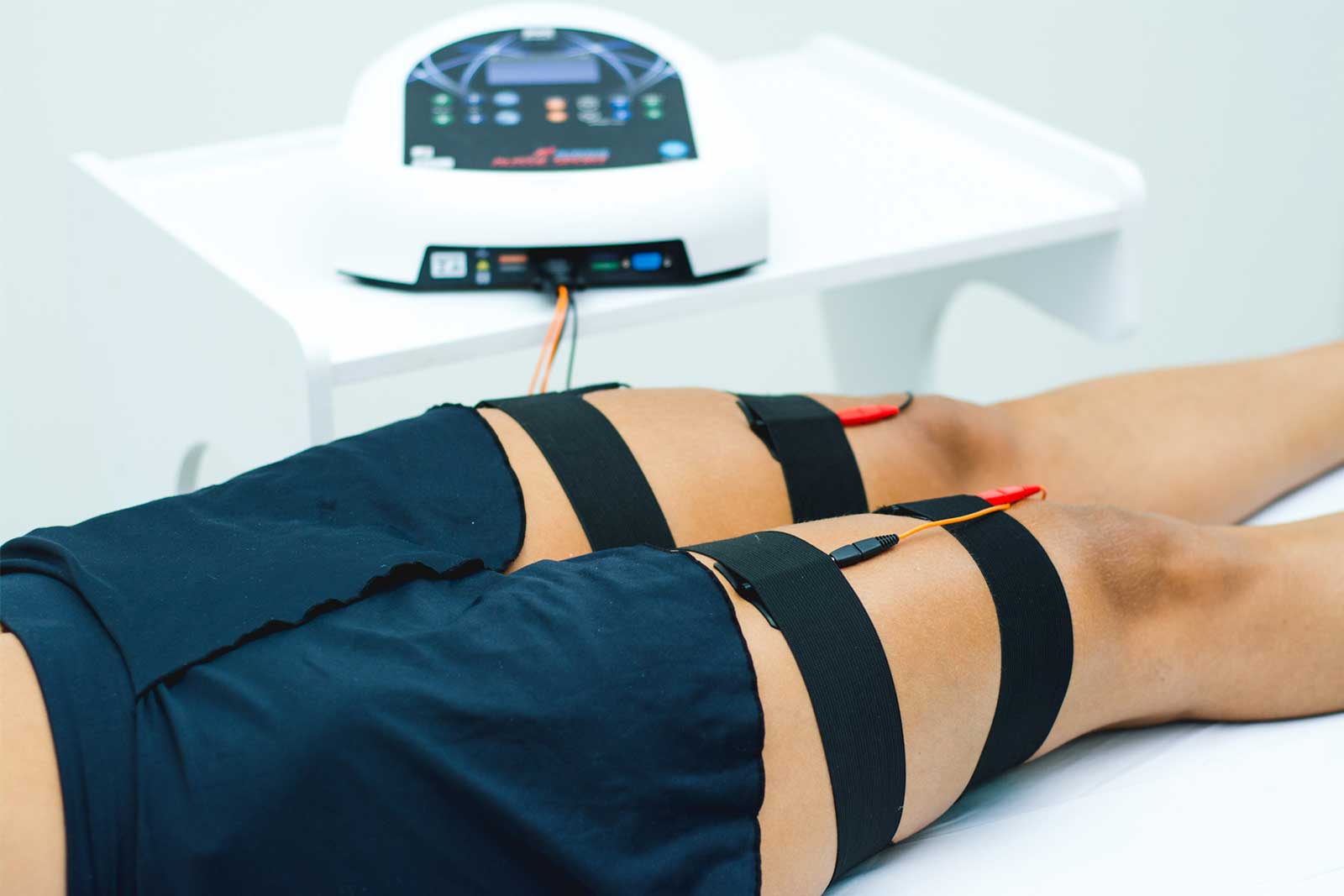
The electrodes placement can be performed using the bipolar or monopolar technique. The adequate positioning and contact of the electrodes will assure comfort and efficacy of the treatment.
Examine the skin and clean the treatment area, disinfecting the skin with rubbing alcohol.
Self-adherent electrodes can be attached directly onto the skin.
Make sure that the entire surface of the electrode is in contact with the skin of the patient, pressing it in place.
Check the electrode contact regularly during the treatment.
Examine the skin again after the treatment.